May is EDS & HSD Awareness Month. EDS stands for Ehlers-Danlos Syndrome and HSD for Hypermobility Spectrum Disorder. They are a group of inherited connective tissue disorders that remain under-diagnosed and under-treated. Case in point: I was diagnosed with hypermobile Ehlers-Danlos Syndrome (hEDS) in January at the age of 65, making sense of decades-worth of unexplained symptoms.
The Ehlers-Danlos Society uses the zebra as a symbol of the EDS/HSD community because there is a saying among the medical community that “when you hear hoofbeats, think horses, not zebras” but, sometimes, there really are zebras. Zebras also each have their unique stripe pattern, in the same way that people with EDS/HSD have their own unique presentation, depending on how their collagen and connective tissue is impacted across different body systems at that particular time in their life. The medical system in the United States and in many other countries tends to divvy medical care to specialists who only look at one body system but connective tissue disorders are easier to recognize if one takes a more integrative approach.
And a fun zebra fact: A group of zebras is called a dazzle, which leads to the Ehlers-Danlos Society saying, “Together, we dazzle!”
As I’ve continued to research hEDS, I’ve been engaging in personal forensic diagnostics. So many things I have experienced in my life make sense now that I know of my genetic inheritence of hEDS. For example, I developed tendon problems in my elbow as a young teen which impacted my abilities as a pianist and organist. When I eventually had to resort to surgery in my thirties, the outcome wasn’t as expected and I had to give up playing. I now understand that this was due to my hEDS inherited collagen defects.
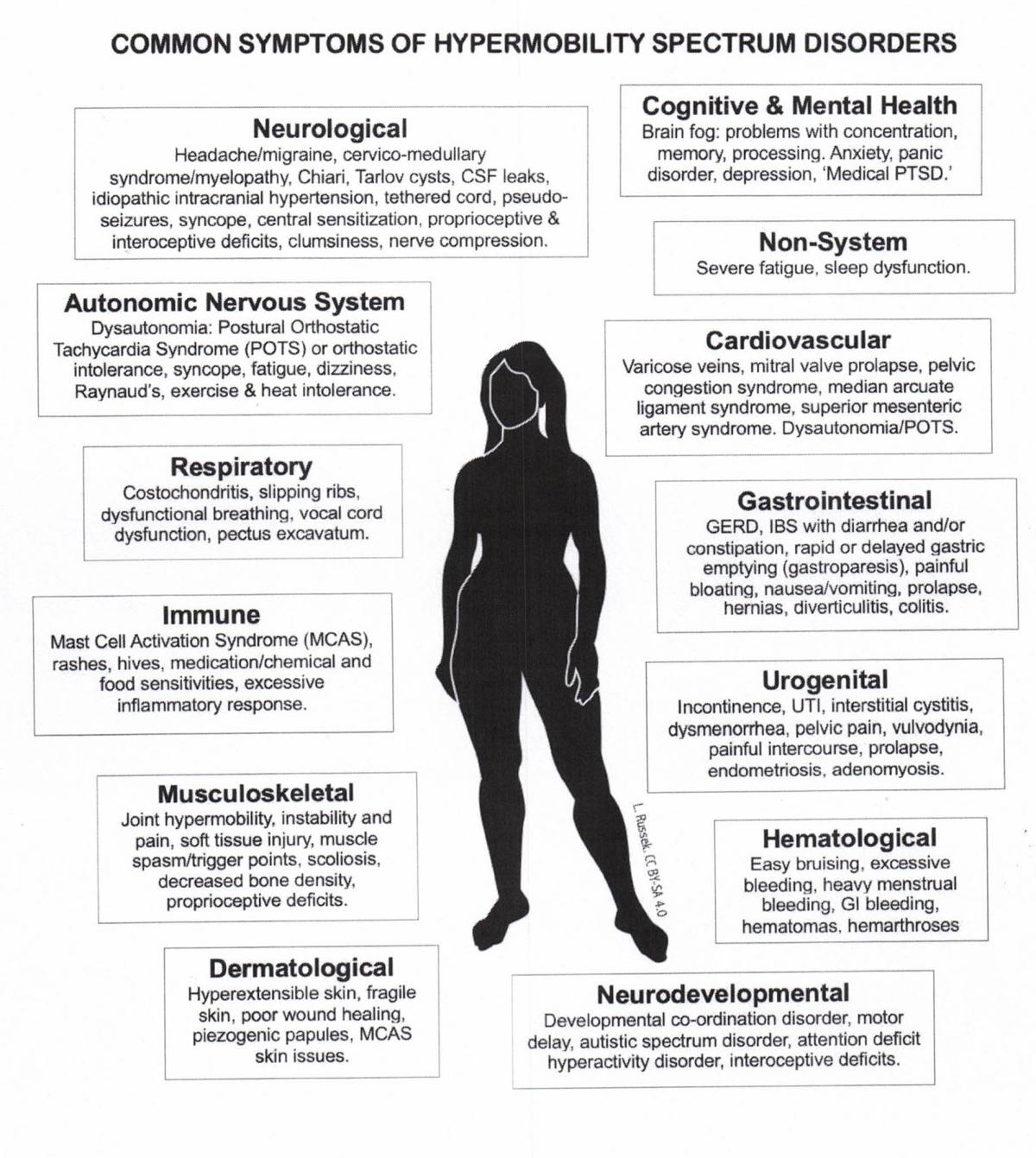
My IBS, IC, endometriosis, vulvodynia, pre-term labor, allergies, mast cell activation disorder, cervical instability, near-sightedness, depression/anxiety, cerebellar ectopia, sleep apnea, early gall bladder disease, hiatal hernia, acid reflux, chronic fatigue, diverticulosis, chronic kidney disease, sensitive skin, joints that bend more than expected, and more all have a connective tissue component and are more likely in people with EDS/HSD.
Daughter T gave me the zebra unicorn pin as a gift. While the zebra is the symbol of EDS/HSD, adding the unicorn element helps to play up the uniqueness of each individual.
And it’s super cute!
The point is that another person with hEDS could exhibit a totally different set of symptoms from mine or we could share some symptoms and not others. It just depends on which connective tissues are compromised and how much at that particular time. Other factors are involved, too, like age, activity level, hormone and endocrine function, etc. It adds to the zebra-unicorn element and takes a thoughtful and informed practitioner to pick up on the possibility of an underlying connective disorder behind all the symptoms of different body parts.
In December, there will be an update to the EDS/HSD diagnostic guidelines. My hope is that the medical community will use these and the best practices guidelines that will follow in spring 2027 to finally look more comprehensively at their patients and diagnose and help them at much younger ages than currently.
Some people are also under the mistaken impression that it doesn’t do any good to give a diagnosis when you can’t cure the disorder. While it’s true that we can’t current treat the genetic cause, there are treatments to help alleviate many of the symptoms. It’s also imperative for practitioners to know the EDS/HSD status for anyone who is contemplating surgery. Surgeons need to know about connective tissue differences so that they can compensate for that during the procedure and the recovery protocols or, perhaps, decide that surgery is not appropriate. Many EDS/HSD patients also need long-term physical therapy to help them function; it makes a huge difference if physical therapists are knowledgeable about connective tissue disorders so that they help rather than hurt.
As I continue my journey with hEDS, I will keep you posted here at Top of JC’s Mind. If we are super-lucky and we find effective treatment for my brain fog and fatigue, I may even post more regularly.
I will, though, always remain my unique, zebra-unicorn self.